
By Brian LaHart, International Workforce Solutions Leader
Direct hire of international nurses carries significant upfront costs — across recruitment, immigration filings, credentialing, and internal resources — that accrue before a single clinician arrives. When timelines shift (and they often do), the hospital absorbs the full financial and operational risk with no guaranteed delivery date. A temp-to-perm model transfers that risk to a partner, with payment beginning only when the clinician starts.
When hospital executives talk to me about direct hire, the conversation almost always starts with cost —specifically, long-term savings. That’s a fair place to start. But after years advising health systems on global staffing strategy, I’ve come to believe that framing misses the real question.
The decision isn’t just about cost. It’s about how much risk, timing uncertainty, and execution your organization is prepared to own.
Why Direct Hire Costs More Than the Invoice Says: Hidden Risks in Hospital Workforce Planning
Direct hire isn’t free, even before a single nurse arrives. It requires significant upfront investment across recruitment, legal work, immigration filings, credentialing, and internal resources — often spanning multiple budget cycles before a clinician ever sets foot in your facility.
That timeline isn’t always predictable, either. Visibility into when a hire will actually arrive is limited, and it can shift over time. The real concern isn’t just the cost itself — it’s what happens if timelines move after that investment has already been made.
That gap between investment and visibility is where pressure builds. What starts as a cost decision quietly becomes a decision about timing, execution, and long-term outcomes. The key difference between workforce models isn’t intent — every model is trying to solve the same problem. The difference is who owns the risk, the timing, and the results.
Who Holds the Risk in Healthcare Staffing? Direct Hire vs. Temp-to-Perm
Direct hire is often evaluated as the lower-cost option on paper. In practice, the real risk isn’t cost alone— it’s when that cost is incurred and how much visibility exists into the outcome.
Hospitals pursuing direct hire commit significant capital before arrival timelines are even clear. If those timelines shift, the investment already made doesn’t shrink — it stays fixed, while delivery moves further out. No part of the process has necessarily failed. But the financial and operational risk sits entirely with the hospital.
At that point, your organization isn’t just waiting. It’s managing a multi-year investment without a predictable timeline for return. I've sat across the table from CFOs inexactly this spot — the project plan looked fine on a slide, and eighteenmonths later they were explaining a stalled headcount line to their board with no better answer than "the visa is still processing."
Hospitals that pursue direct hire also take on full responsibility for:
• Sponsorship, immigration filings, and legal coordination
• Tracking visa movement and timeline changes
• Managing multi-year candidate engagement
• Overseeing credentialing, licensure, and compliance
• Supporting relocation and early integration
• Carrying the upfront financial exposure
Direct Hire vs. Temp-to-Perm, Side by Side
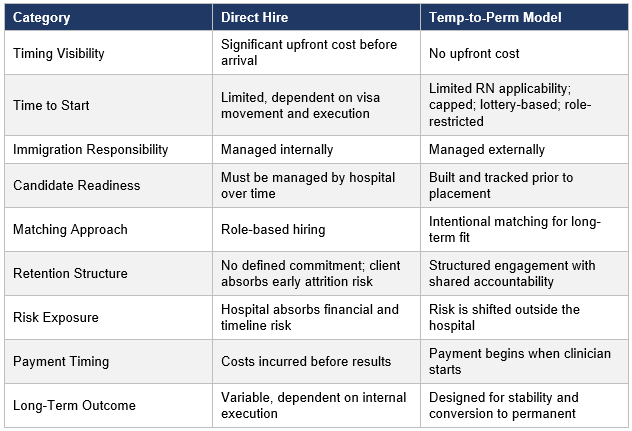
How a Shared-Risk Workforce Model Produces More Predictable Healthcare Staffing Outcomes
The alternative to direct hire isn’t a more comprehensive version of the same approach — it’s a fundamentally different model, built to deliver consistent workforce outcomes through Direct hire, by contrast, relies far more heavily on internal capacity for preparation, integration, and retention. That’s where early attrition risk can reset both cost and workforce stability in one move. If a clinician leaves early, the hospital absorbs the full impact — after already investing significant time and capital. In a partnership model, that same risk is contained through shared accountability instead of sitting entirely on one side. large-scale, multi-year programs.
In a structured temp-to-perm model, the work begins long before a hospital ever selects a candidate. Pipelines are actively managed in advance, with clinicians progressing through immigration, preparation, and readiness milestones well ahead of placement. Matching is intentional — not just by role, but by environment and long-term fit, aligning clinician preferences with the needs of the facility and the surrounding community.
That foundation, paired with a defined commitment period and continued support after arrival, is what drives workforce stability and strong conversion to permanent employment.
There’s no upfront cost in this model. Payment begins only when the clinician is actively working, backed by a multi-year engagement that gives you clear visibility into cost and a defined path to permanent placement.
This model changes the workforce equation:
• No upfront cost or sunk investment risk
• Pipeline already in motion
• Greater visibility into timing
• Clear alignment between investment and delivery
• Structured, multi-year engagement
• Immigration and timeline risk managed externally
• Structured preparation, onboarding, and integration support
The Real Question for Hospital Workforce Planning
Direct hire is not inherently the wrong choice. But it’s a model that requires infrastructure, time, capital, and sustained execution — often with significant investment made well before outcomes are visible.
The real question isn’t whether direct hire can work. It’s whether your organization is prepared to invest early, manage uncertainty, and sustain execution over multiple years —or whether you’d rather choose a model that offers clearer visibility and a defined path to workforce stability from day one.
Travel staffing solves for temporary disruption. Long-term workforce stability requires a different strategy entirely.
Frequently Asked Questions
What is the difference between direct hire and temp-to-perm for international nurses?
In a direct hire model, the hospital sponsors the nurse's immigration, manages the process internally, and absorbs all upfront costs and timeline risk before the clinician ever arrives. In a temp-to-perm model, a staffing partner manages immigration end-to-end as the employer of record, and the hospital pays only once the clinician starts —with a structured pathway to permanent placement built in from the beginning.
How long does direct hire of international nurses typically take?
Direct hire of internationally-educated nurses typically involves a multi-year process spanning recruitment, immigration filings, visa processing, credentialing, and relocation — often two to four years from initiation to arrival. Timelines are heavily dependent on visa bulletin movement, country of origin, and the hospital's internal capacity to manage the process.
What are the upfront costs of direct hiring international nurses?
Upfront costs include immigration attorney fees, visa filing fees, recruitment expenses, credentialing and licensure costs, and internal staff time for ongoing candidate management and compliance. These costs are incurred before the nurse arrives and before any workforce impact is realized — and they remain fixed even if timelines shift.
Which international nurse staffing model carries less financial risk for hospitals?
The temp-to-perm model carries significantly less financial risk for hospitals. There is no upfront cost or sunk investment — payment begins only when the clinician starts working. Immigration liability, filing responsibilities, and timeline risk are all managed externally by the staffing partner rather than absorbed by the hospital.
What is temp-to-perm nursing staffing and how does it work?
Temp-to-perm nursing staffing places internationally-educated nurses on multi-year contracts managed by a staffing partner who serves as the employer of record. During the contract period, the partner handles immigration, credentialing, onboarding support, and ongoing retention. At the end of the engagement, nurses are structured to convert to permanent employment at the hospital.
Can a hospital switch from direct hire to a temp-to-perm international staffing model?
Yes. Many health systems transition from direct hire to a partnership model when internal immigration management becomes operationally burdensome or when timeline uncertainty creates budget risk. The transition typically involves partnering with a staffing organization that already has an active pipeline of candidates in process, allowing for faster access to candidates without restarting immigration from scratch.
About the Author
Brian LaHart is Health Carousel's International Workforce Solutions Leader, an international workforce leader with extensive experience advising hospital executives on global staffing strategy and workforce planning.


