
By Brian LaHart, International Workforce Solutions Leader
Many hospitals have reduced traveler utilization since the pandemic peak — but overall hospital labor costsremain significantly elevated, because organizations replaced contingent laborwith higher permanent wages and expanded premium pay. The operational pressurehasn't eased; it changed form. Understanding the difference between temporarystaffing gaps and structural workforce shortages is now the central workforceplanning challenge for hospital leadership.
Across healthcare, staffing metrics are improving. Traveler utilization and vacancy rates have declined,and some organizations are seeing lower census volumes. Compared to the heightof the workforce crisis, many leadership teams feel more stable.
Yet many organizations continue facing operational and financial pressure. Clinical leaders still rely onovertime, incentives, and contingent labor to maintain staffing coverage, evenas traveler spend declines.
The challenge facing leadership today is more nuanced: how to reduce labor spend without creating additional strain on clinical teams delivering patient care every day. Many organizations appear appropriately staffed on paper while still struggling operationally underneath, because workforce health is not reflected by vacancy rates alone. Many systems today are staffed to budget — but not consistently staffed to actual demand.
“Organizations may be staffed to budget — not actual demand. Metrics may improve, but the operational reality remains untenable for many.”
Hospital Labor Costs and Traveler Utilization: Why Lower Contingent Labor Spend Hasn't Solved the Problem
The staffing problem did not disappear — it changed form.
Traveler utilization has declined from peak pandemic levels, but many organizations reduced traveler reliance by increasing RN wages, bonuses, and premium pay. Those decisions improved staffing stability while permanently resetting labor costs to a higher baseline. Traveler utilization has declined, but labor costs remain elevated.
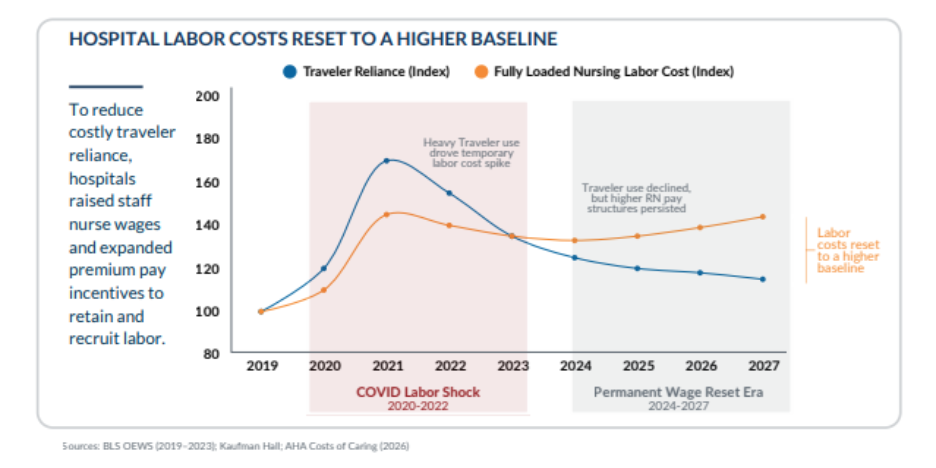
During the COVID labor shock of 2020–2022, heavy traveler use drove a temporary labor cost spike. In the years since — what the original analysis calls the "Permanent Wage Reset Era" of 2024–2027 — traveler use has declined, but the higher RN pay structures organizations put in place to reduce that traveler reliance have persisted. The net effect: labor costs reset to a higher baseline that hasn't come back down even as travel staffing usage has.
I talk to CFOs who point to their traveler-spend chart as proof the worst is over, and then in the same meeting, their CNO is asking for more overtime approvals. Both things are true. That's the disconnect.
The challenge is no longer reducing travelers. The challenge is determining where contingent labor is still serving a short-term operational purpose versus where it has become embedded into ongoing workforce operations.
Healthcare organizations must determine:
- Which staffing gaps are temporary versus structural
- Where premium labor has become operationally embedded
- Which roles represent chronic workforce shortages
- Whether schedules can be consistently staffed without ongoing workarounds
The workforce conversation has shifted from crisis response to sustainable workforce design.
Temporary Flexibility vs .Structural Shortage: How High-Performing Health Systems Are Rethinking Contingent Labor Strategy
The goal is not eliminating travel staffing, but using it more intentionally within a sustainable workforce model.
High-performing organizations increasingly separate short-term operational flexibility needs from long-term structural workforce shortages. In this approach, travelers continue supporting temporary disruptions, while repeatable staffing gaps transition toward permanent workforce capacity through long-term workforce planning and internationally-educated clinicians.
That distinction changes both operational and financial outcomes. Organizations gain:
• More predictable staffing coverage
• Reduced reliance on reactive premium labor
• Improved workforce planning visibility
• A more sustainable long-term labor model
Rather than using travelers indefinitely in repeatable roles, organizations can gradually build permanentworkforce supply into areas experiencing chronic shortages — creating a morebalanced approach between flexibility, financial sustainability, and operational stability.
The opportunity is no longer simply traveler reduction. It's building a workforce model capable of sustaining clinical operations without permanently escalating labor costs.
The Real Measure of Hospital Workforce Health in 2026 and Beyond
Healthcare organizations have made meaningful progress since the peak workforce crisis years. But improving staffing metrics alone does not necessarily mean the workforce challenge has been solved. The challenge facing health systems today is no longer emergency staffing response — it's balancing financial sustainability with consistent clinical coverage over time.
The question is no longer whether staffing metrics look better. The question is whether the workforce strategy supporting them is durable enough for the future.
Frequently Asked Questions
Why are hospital labor costs still high if traveler nurse utilization has declined?
Hospitals reduced traveler reliance by raising permanent RN wages, expanding sign-on bonuses, and increasing premium pay incentives — decisions that stabilized staffing but permanently reset the fully loaded cost baseline upward. Traveler spend declined, but the higher permanent compensation structures put in place to replace that spend persisted, leaving total nursing labor costs elevated even as contingent labor usage fell.
What is the difference between a temporary staffing gap and a structural workforce shortage?
A temporary staffing gap is a short-term vacancy created by leave, census surge, or turnover in a role that can be filled quickly and stabilized. A structural shortage is a chronic, repeatable gap in a role or specialty where the local talent supply is consistently insufficient to meet demand without ongoing premium labor. Hospitals managing structural shortages with travelers indefinitely are solving a permanent problem with a temporary — and expensive — tool.
What is contingent labor dependency and why is it a financial risk for hospitals?
Contingent labor dependency occurs when roles that were originally filled with travelers for short-term flexibility become operationally reliant on ongoing traveler coverage — can't be consistently staffed without them. This creates a recurring premium labor cost in roles where the gap is structural, not temporary, which permanently elevates the labor cost baseline and reduces financial predictability for hospital leadership.
How can hospitals reduce traveler reliance without creating staffing gaps?
The most effective approach is to separate temporary flexibility needs from structural shortages, then build permanent workforce supply into the structural roles through long-term workforce planning — including internationally-educated clinicians on temp-to-perm pathways. This allows travelers to serve their actual purpose (short-term disruption coverage) while reducing the chronic, repeatable dependency that drives unsustainable labor costs.
What metrics should hospital leaders track to evaluate true workforce health beyond vacancy rate?
Vacancy rate alone is an insufficient measure of workforce health. Leaders should also track overtime hours and trend direction, premium pay spend as a percentage of total labor cost, the ratio of temporary to permanent staffing in chronically short roles, schedule fill rate without workarounds, and whether contingent labor usage is declining, stable, or growing in specific units or specialties.
What is sustainable hospital workforce planning and how does it differ from crisis staffing response?
Sustainable workforce planning separates short-term operational flexibility from long-term structural supply strategy, builds permanent workforce capacity in chronic shortage areas through international and domestic pipelines, and reduces recurring premium labor dependency over time. Crisis staffing response fills immediate vacancies —usually with travelers — without addressing the structural conditions that created the gap, resulting in ongoing cycle of premium labor reliance.
About the Author
Brian LaHart is Health Carousel's International Workforce Solutions Leader, an international workforce leader with extensive experience advising hospital executives on global staffing strategy and workforce planning.


